Healthcare
News and insights on healthcare IT technology that can impact patient outcomes, care, accessibility, security, and compliance. Healthcare IT technology is evolving fast, especially as organizations have geared up for technologies such as electronic health records, telemedicine and healthcare interoperability standards such as FHIR. Healthcare organizations must also pay close attention to security, compliance, the cloud, and analytics and AI. This section provides news and insights into the technology behind Healthcare IT including software and tools, organizational strategies, and innovative use cases.

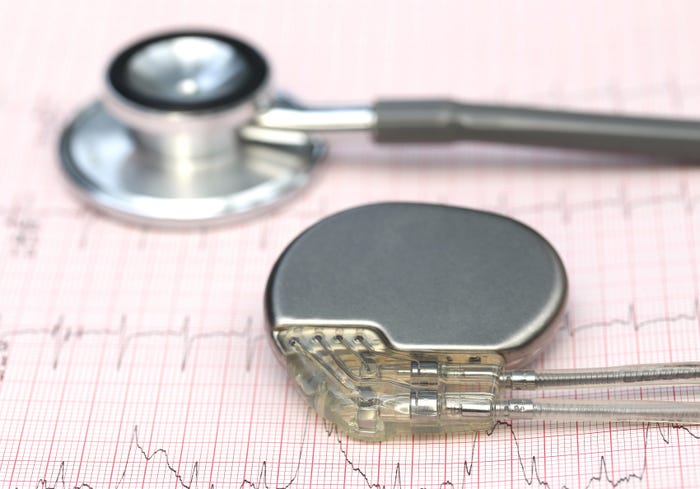
Contactless technology is a form of remote health monitoring that uses AI to analyze vital signs, facial expressions, facial blood flow, or vocal behavior to detect medical issues faster than a more invasive physical exam.